2. How can the level of virus REPLICATION be determined?
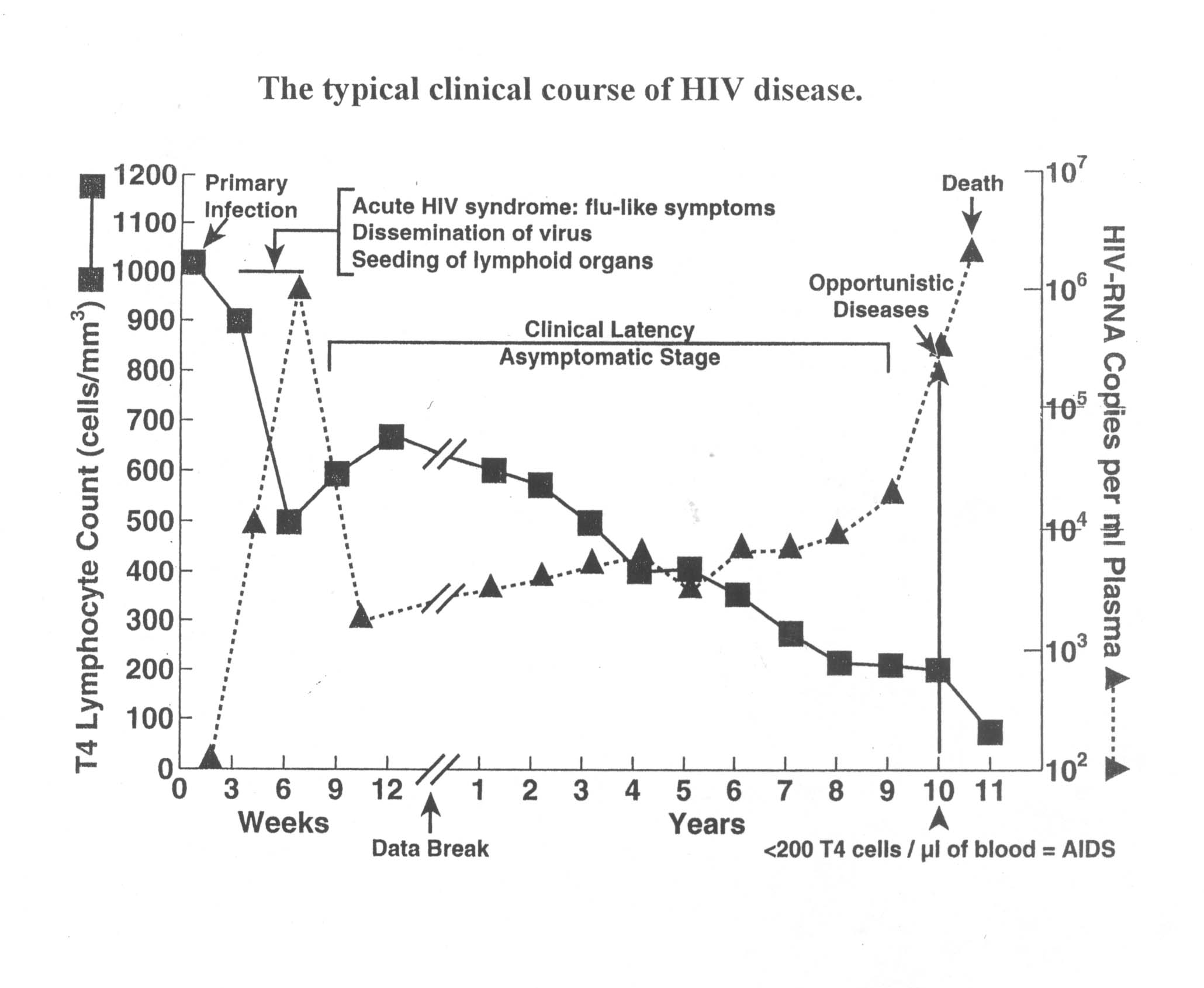
For an infected individual in the long asymptomatic stage, the Figure above gives us an approximate value for the concentration of HIV in the person's blood (the "viral load"), but does not tell us the turnover rate (how many new virions were produced "yesterday"). A roughly constant viral load results whenever the virus replication rate and the virus destruction/elimination rate are essentially balanced.
The turnover rate was first measured in a series of experiments starting in 1995 by a research team headed by Dr. David Ho (who is now head of the Aaron Diamond AIDS Research Center in New York), as part of the clinical trials that led to the approval of the protease inhibitors. Because these drugs act so quickly and powerfully to prevent production of new virions, but do not destroy virions that already exist, investigators could start a person on the drug, and then measure how quickly the viral load in the person's body dropped (due to natural destruction/elimination). This "negative" rate is then taken as a measure of the "positive" rate of virus replication normally going on in the person's body, because these two rates have to be equal for there to be a constant steady state viral load. ((An analogy is any body of water with water flowing in and out at equal rates, and thus the water level staying constant. Stop the in-flow, let the out-flow continue, and measure how fast the water volume in the container drops. This gives you a measure of the original in-flow rate.))
3. What IS the level of virus replication in a typical HIV+ individual?
We know that a typical viral load is somewhere around 10E4 virions/ml of blood plasma.
When a patient is started on protease inhibitor treatment, there is typically a 100 fold drop in viral load in 7-10 days. Mathematically, this is an exponential drop off with a "half-life" of about one day.
So, what does this say about what is happening normally (w/o drug therapy)?
Every day in an HIV+ individual with a typical viral load, about 5 thousand or so new virions are being produced per ml of blood. In the body as a whole, perhaps a hundred million (or so) new virions are being produced every day. Essentially ALL of the virions present in the blood at any time were produced within just the past few days.
This means that there are over 100 generations (successive replication cycles) of HIV per year in a person's body. Virus at the end of a ten year infection is more than a thousand generations removed from the initial virion that started the infection in the person a decade earlier.
The body's CD4+ T lymphocytes ("T4" cells) are being continually infected and being killed during this long process of high virus replication. Perhaps a hundred million or so of the body's 100 billion or so T4 cells get infected each day, and die within a couple of days. This ongoing (day after day after day after day.....) situation puts an extra heavy burden on the body's T4 replenishment ability. The continual stress on the body to be producing extra T4 cells eventually leads to a break down in the ability to keep making enough of these cells for proper functioning of the immune system.