Until the mid 1990's, the extent of HIV replication going on in a typical HIV+ individual was not clear. Because of the long asymptomatic period that can last for at least several years, it had been thought that there was a very low level of virus replication for a number of years, with the very slow killing of T4 lymphocytes (CD4+ Th cells). Studies were hindered by the fact that it was not possible to accurately measure the actual concentration of HIV (the "virus load") in a person's blood, and there was also no way to measure how rapidly these viruses are replicating. Early during the 1990's it became possible to measure accurately the levels of HIV in a blood sample by quantitative assays for viral RNA concentration, and then in 1995 it became possible to measure the viral replication rate.
1. What is the typical clinical course of HIV infection in a person?
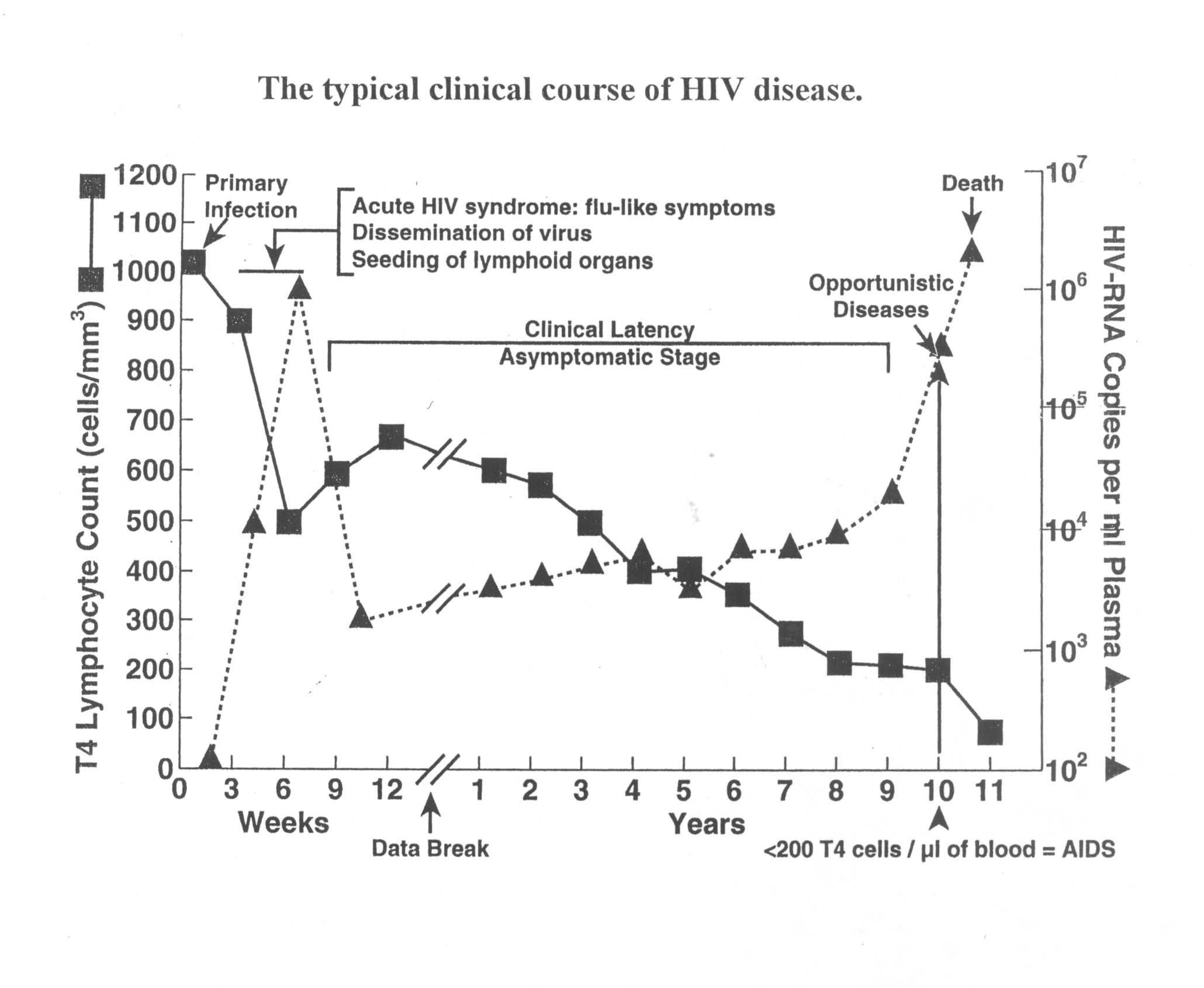
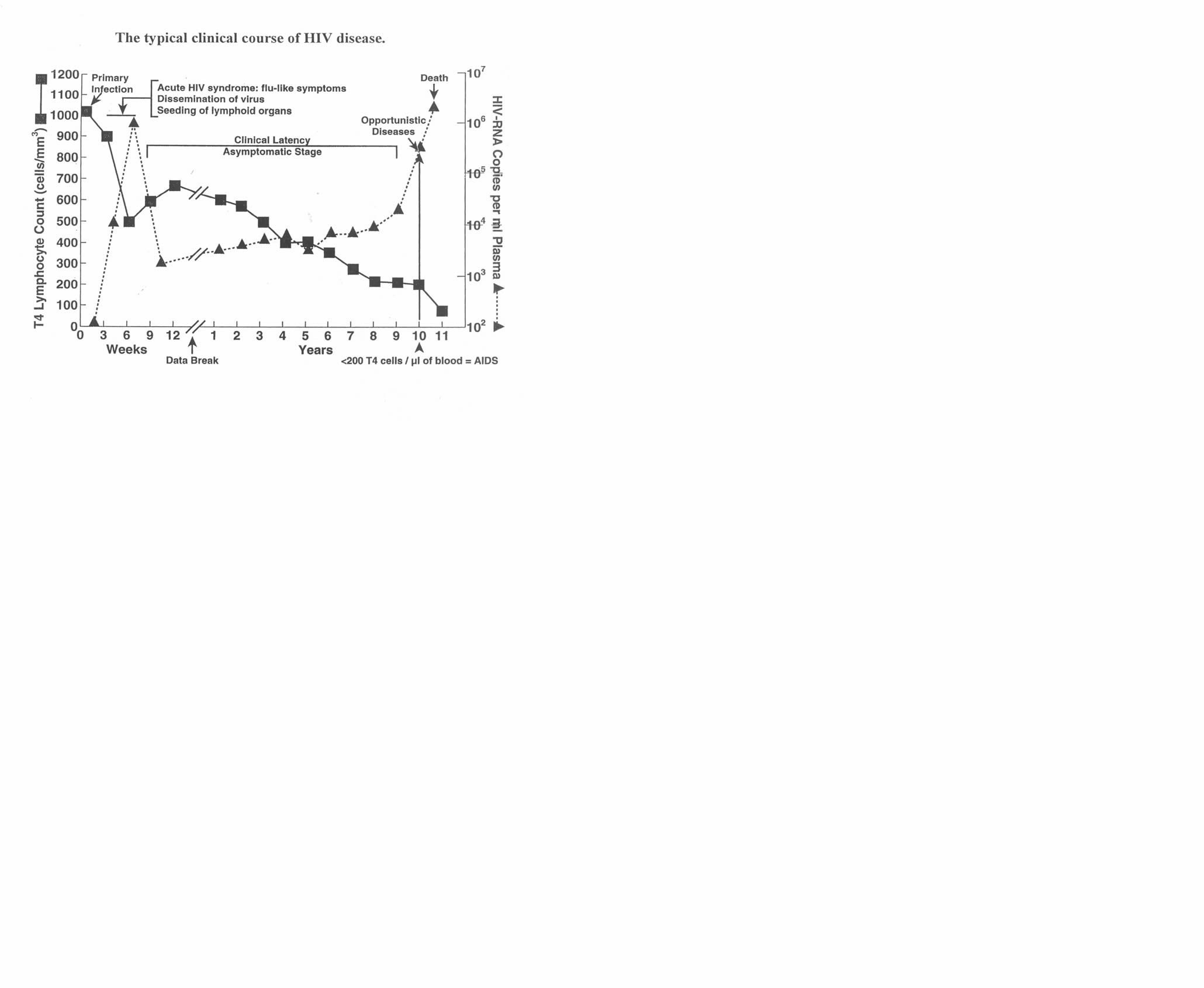
Once the technology for measuring viral load was in place, a number of studies showed that a typical clinical course of HIV infection over a ten or so year period can be graphed as shown here or here. (Figures are the same but size may be browser-dependent, and you may need to print in "landscape" mode. Adapted from a review article by Anthony Fauci, head of the National Institute of Allergy and Infectious Diseases).
2. What is the level of virus replication in a typical HIV+ individual?
A typical viral load is somewhere around 10,000 virions/ml of blood plasma. When a patient is started on protease inhibitor treatment, there is typically a 100 fold drop in viral load in about 10 days. Mathematically, this is an exponential drop off with a "half-life" of about one day, and this provides a measure of the normal turnover rate. That is, about half the virions in a person's blood are ones that were produced within the past day or so.
So, for someone (not on antiviral drug therapy) with a viral load of 10,000 virions/ml, about 5 thousand or so new virions are being produced per ml of blood per day. In the body as a whole, perhaps a hundred million (or so) new virions are being produced every day. Essentially all of the virions present in the blood at any time were produced within the past week or so.
At least a few million CD4+ T lymphocytes ("T4 cells") get infected each day, and die within a couple of days. This ongoing (day after day after day after day.....) situation puts an extra heavy burden on the body's T4 replenishment ability. The continual stress on the body to be producing extra T4 cells contributes to a break down in the ability to keep making enough of these cells for proper functioning of the immune system.
3. How is the situation different for an HIV+ individual who is on effective anti-HIV drug therapy?
If the person is on effective anti-HIV drug therapy, the amount of virus replication is greatly reduced. In some cases, the level of replication gets so low that, within the limits of the measurement technique, no virus load can be detected in the person's blood. With very little virus replication going on, the number of T4 cells being killed each day is also very low, so the "replenishment stress" on the immune system is also low.
So, from a clinical perspective, it may almost seem as if the person is cured. However, many studies have shown that there are always "reservoirs" of virus and infected cells in the lymph nodes and among memory T cells. So, even though no virus may be detectable in the blood, the person is definitely not virus-free. If the drug-therapy that has been "effective" for an extended period of time starts to fail, the viral load will start to rise again.
4. How many virions with mutant genomes are being produced each day?
The HIV replication cycle is such that mutations can occur at two stages of virus replication: first, at the level of the synthesis of the ds DNA copy of the viral RNA genome by reverse transcriptase, and second, at the level of the synthesis of new full length RNA genomes from the ds DNA by cellular RNA polymerase. Since neither of these enzymatic processes has proof-reading capability, there ends up being about one random base change somewhere in most new copies of the HIV genome that get made.
With a hundred million (or so) new virions being produced each day, it is clear that all possible point mutations occur every day. In addition, RNA recombination processes provide a mechanism for increased variation.
5. What happens as natural selection acts on this genetically diverse population?
So, there is a large, genetically diverse population of HIV in the person's body every day, with rapid turnover giving over a hundred generations per year. Given these numbers, we might expect to see noticeable viral evolutionary change within an individual.
In general, there will be enhanced replication of mutants that can somewhat evade immune system recognition or replicate in a wider range of host cells. (Regarding the last of these, it is almost always observed that the virus population eventually acquires the ability to use several other co-receptors, not just CCR5. In addition, sometimes the virus even acquires the ability to use molecules other than CD4 as primary receptor.)
The ever-expanding genetic diversity of the virus means that the immune system has to keep working almost as if a brand new virus infection is starting every month or so. For example, B cells that were clonally selected a month or so ago in an HIV+ person may be losing their effectiveness, because random HIV mutants with a gp120-gp41 glycoprotein structure that the antibodies can't quite recognize as well have been replicating at a higher rate in the body. Likewise, Tc cells clonally selected at an earlier time lose their effectiveness due to viral evolutionary change. For example, a 2004 article by Leslie et al., in Nature Medicine begins with the sentence "Within-patient HIV evolution reflects the strong selection pressure driving viral escape from cytotoxic T-lymphocyte (CTL) recognition."
Both arms of the immune response are under continual stress due to viral evolutionary divergence, and meanwhile, as the infection proceeds, the virus is killing millions of CD4+ T lymphocytes per day, putting additional stress on an already stressed system. Eventually, the T4 cell counts get very low ( less than 200 T4 cells per ul ) and the overall system starts to collapse in the manner characteristic of the onset of full-blown AIDS.
{kind=link}
{kind=link}